From OpenAI to self-hosted: why healthcare AI doesn't belong in a Golden Cage
Building a chatbot is the easy part. The real questions come afterwards: where does the model run, and who owns the data? In healthcare those aren’t implementation details. They’re the whole question.

1. The problem isn’t intelligence. It’s trust.
People with a chronic condition have questions — a lot of them. About food, exercise, sleep, stress. They ask Google, a forum, ChatGPT. And they get answers that range from incomplete to outright dangerous.
It’s tempting to think a smarter model solves that. It doesn’t. The largest language models in the world are brilliant and unreliable at the same time: they sound just as convincing when they’re right as when they make things up. In most applications that’s annoying. In healthcare it’s dangerous.
So the bottleneck isn’t the intelligence of the model. It’s the traceability of the answer. And that’s not a model problem — it’s an architecture problem. That’s where the story of Lampie, our AI lifestyle assistant, begins.
2. The architecture: RAG on a dense, validated source
Lampie isn’t a model that “knows whatever it happens to know”. It’s built on RAG — Retrieval-Augmented Generation. The principle: don’t let the model talk from memory; let it first search a bounded, trusted source and only then answer based on what it found.
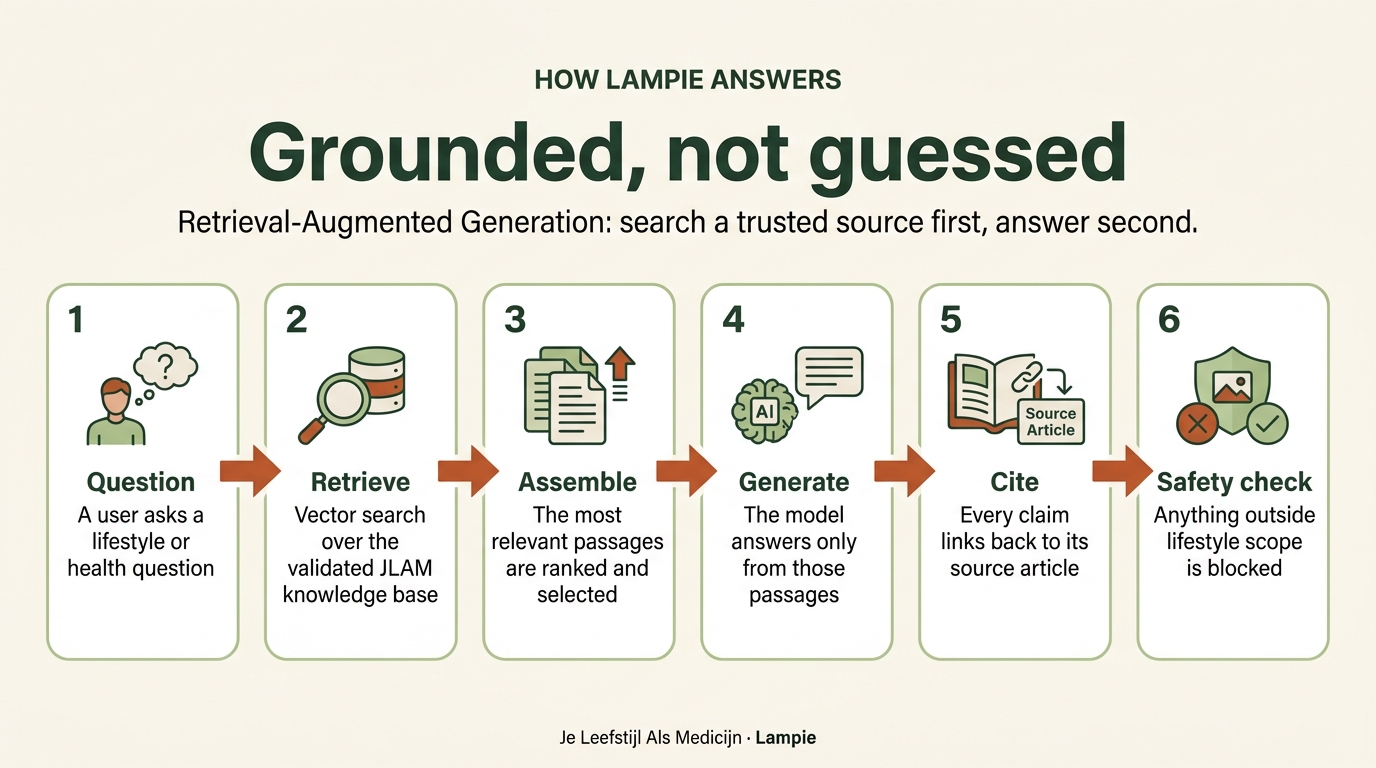
The difference with “just ask ChatGPT” lives in two places: retrieval and citation. Lampie doesn’t draw on the open internet but on one bounded source: hundreds of articles written and reviewed by medical professionals, based on guidelines — the Dutch NHG and FMS, and internationally the CDC, MedlinePlus and the NHS — supplemented with the Lifestyle Coalition’s knowledge bundle, Voeding Leeft, Kanker.nl, the Trimbos Institute and the Dutch Health Council’s exercise guidelines. On top of that Lampie knows more than 5,500 local lifestyle locations and over 1,750 recipes with full nutritional data.
Every claim is traceable to a specific article. No hallucinations on medical topics — not because the model is well-behaved, but because the architecture enforces it.
3. The guardrail lives in the core logic, not the footer
“Lampie gives lifestyle advice, not medical advice.” That’s not a disclaimer at the bottom of the page. It’s a design rule built into the core.
What’s technically interesting is how. We use an intermediate compliance layer: an agent that sits between the language model and the user and filters the output, so that lifestyle advice remains and medical claims or diagnoses don’t. The user gets an answer that stays inside the lines; for a medical question Lampie explicitly refers on to a healthcare professional.
This is the same idea I described in The Vault and the Poet: you decouple the creative, unpredictable part (the language model — the poet) from the part that has to be strict (the rules — the lock). The model may phrase; a separate layer guards what’s allowed out. In healthcare that separation isn’t a luxury but a requirement. It’s no coincidence that Lampie falls under the “limited risk” category of the EU AI Act.
4. Privacy by design: the data we deliberately don’t want
Most AI products want to know as much about you as possible. Lampie is designed the other way round: it deliberately does not want your data.
- No login, no account, no app.
- It doesn’t ask for your name, email or phone number.
- If you do accidentally share personal data, it’s automatically stripped from the stored messages — via Google Cloud Sensitive Data Protection (DLP).
- Conversations are automatically deleted after a maximum of 365 days.
- And you always know you’re talking to an AI.
The less we keep, the less can leak. Privacy here isn’t an afterthought but a design principle. And it brings me to the heart of this piece — the question of where the model itself runs.
5. Out of the Golden Cage: why we’re moving to our own models
Today Lampie runs on a bought-in model. We started on OpenAI and are now moving increasingly towards Claude. That works — but it’s not where we want to end up. The course is clear: towards our own, self-hosted models.
To explain why, I’ll borrow an argument from Jan Baan — the man who built ERP giant Baan Company. His observation about modern software: the SaaS model locks an organisation’s unique logic into a proprietary “Golden Cage”, and makes you pay an ever-rising “Runtime Tax” for it — subscription plus usage, endlessly. The real winners, Baan says, don’t just make work disappear; they give organisations ownership of their outcomes. Away from vendor lock-in, from renting (OPEX) to owning (CAPEX).
Baan is talking about booking data into your ERP. But exactly the same holds for healthcare systems — only heavier. Because here it isn’t about ledger lines, but about patient data: the most sensitive there is. A care organisation that rents its AI lets its patients’ questions — about their health, their fears, their bodies — run through another company’s Golden Cage, on a cloud it has no say over. And the moment that data passes through a rented model, you share it with a third party — often an American one, and thus under the US Cloud Act. In healthcare, owning your model and your data therefore isn’t cost optimisation. It’s a precondition for trust.
That’s why self-hosted, for us, isn’t a technical preference but a principle. As long as the model belongs to someone else, you’re a guest in their cage. Our own, self-hosted models mean sensitive patient data never leaves our own house — and never ends up in an American model. It’s the same conviction that runs through everything I build: that you should be in charge of your own health — and of your own data.
6. From our own site to the waiting room
Lampie is a product of our foundation itself, built in partnership with the Dutch AI startup AI voor Impact — with us as the commissioning client, not the buyer of an off-the-shelf package. It has run in the bottom-right corner of every page of our own website since 2024. But the interesting part only started when others wanted it.
Technically, Lampie is an embeddable widget: a care institution puts it on its own site, keeping its own branding, and gets a dashboard with insight into what visitors are searching for. One shared, validated knowledge base underneath; many front doors on top.
In October 2025 the Elkerliek hospital in Helmond became the first Dutch hospital to integrate Lampie. Care-innovation lead Elske Berkvens — originally a physiotherapy scientist — was honest about it: it took eleven months. And the time did not go into the technology. It went into proving and documenting that privacy and safety are guaranteed, that Lampie only talks about lifestyle, and that it relies on trusted sources. Exactly the things from the previous chapters — in contract form.
That’s the real pioneering work. Elkerliek drafted those agreements so that other institutions can pick them up directly. They have, in Berkvens’ words, “cleared the path.” And on 1 June 2026 the first follower arrived: DC Klinieken went live with Lampie in twelve languages — led by Cecile Goldman-Corbeij, director of Innovation & Digitalisation, and medical lead Lian Tjon Soei Len. Not a hospital but a chain of independent clinics, which immediately proves the model works beyond one type of institution. By now Lampie has answered more than 15,000 questions.
7. Why this is Smart Health Communities
A chatbot in a waiting room isn’t big news in itself. It becomes big when you see where it sits in a larger picture.
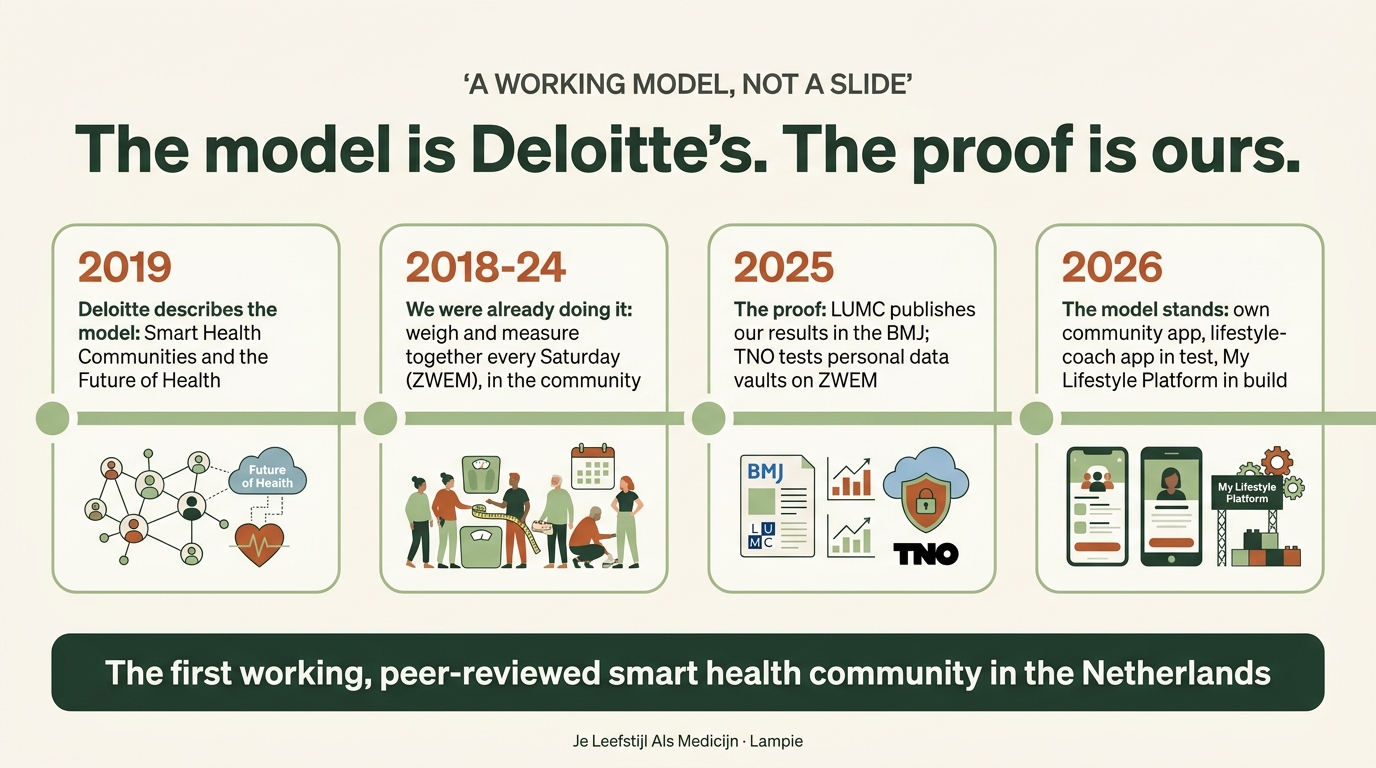
That picture is called Smart Health Communities, the model Deloitte described in 2019 as the future of healthcare. Its uncomfortable premise: roughly 80% of our health is determined outside the consulting room. The community, not the clinic, is the engine of behaviour change. The model rests on five elements — and at our place every element already runs.
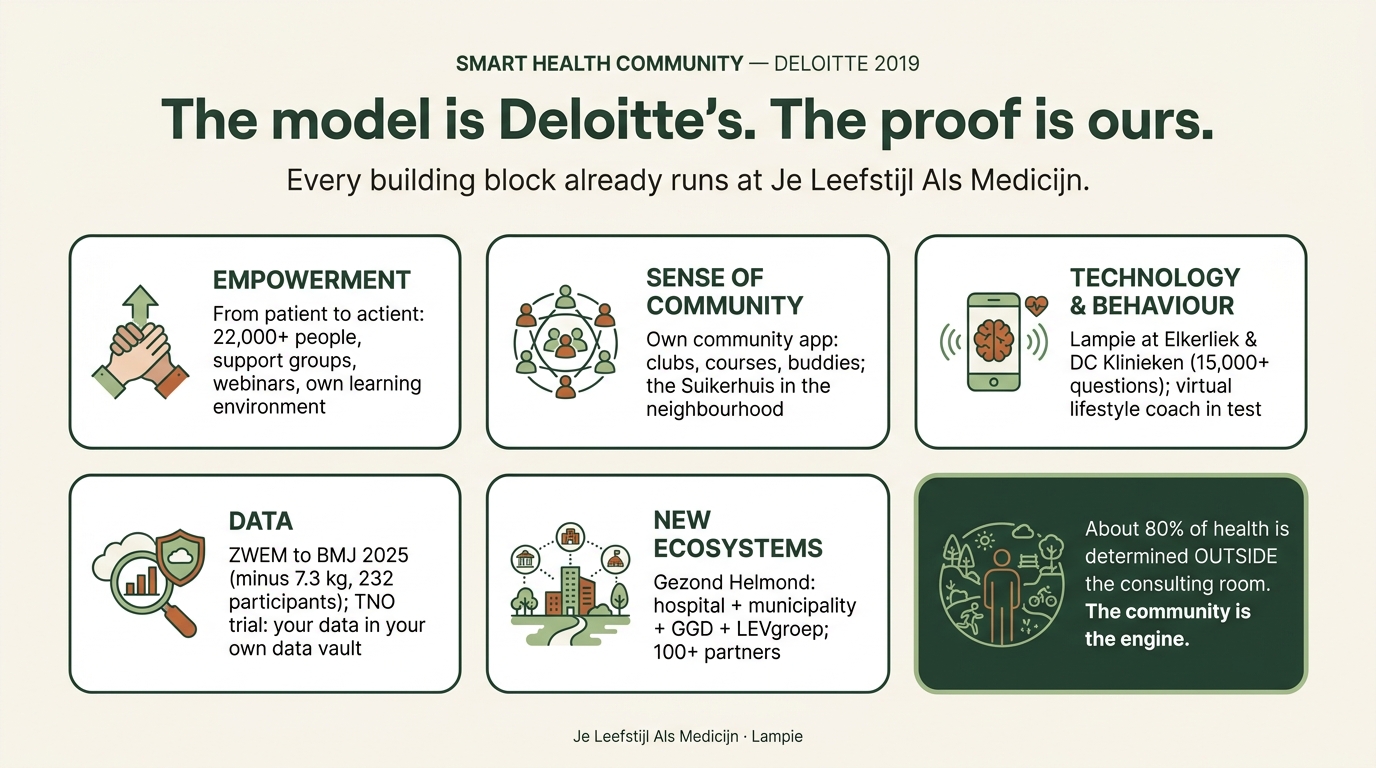
Lampie lands squarely on two of those five. It’s technology that makes reliable knowledge available 24/7 without a doctor between you and the answer. And it’s an ecosystem connector: with those 5,500+ local referrals it’s not an endpoint but a signpost — to the lifestyle coach around the corner, the walking group, the dietitian. By sitting on a hospital’s website, it ties the clinic to the physical ecosystem of the neighbourhood, like Gezond Helmond with its 100+ partners.
And the data building block hits the very heart of this piece. Every Saturday our members measure their weight, waist and blood sugar — ZWEM — which led to our BMJ publication in 2025 (−7.3 kg across 232 participants). In a trial with TNO we’re now adding a personal data vault: your data, in your own vault. That’s exactly the data side of the Golden Cage from chapter 5 — ownership, not rent.
Seen this way, this is exactly the third route I’ve been arguing for: not the purely clinical one (like Virta Health), not the purely commercial one, but the community-driven approach — peer-reviewed and validated, for a fraction of the cost. Lampie isn’t the heart of it. Peer support is the heart. But Lampie makes that route scalable.
8. The next layers: from information to control
Lampie can do a lot, but one thing deliberately not: it doesn’t know you. It’s anonymous and gives general information. That’s a strength — low-threshold and safe — but also a limit. General information doesn’t change behaviour. Guidance does.
So we’re building it as a layered architecture. Four steps:
- Lampie — anonymous lifestyle information, for everyone. Live.
- The virtual lifestyle coach — a personal app that guides you daily on food, movement and sleep; working towards multiple specialists in one coach and integration with sensors such as a glucose monitor, together with TU Delft and the University of Twente. Now in testing with users.
- The digital twin — a digital model of your body that predicts how you respond to food. In development as graduation research.
- A personal health agent — that brings all the threads together.
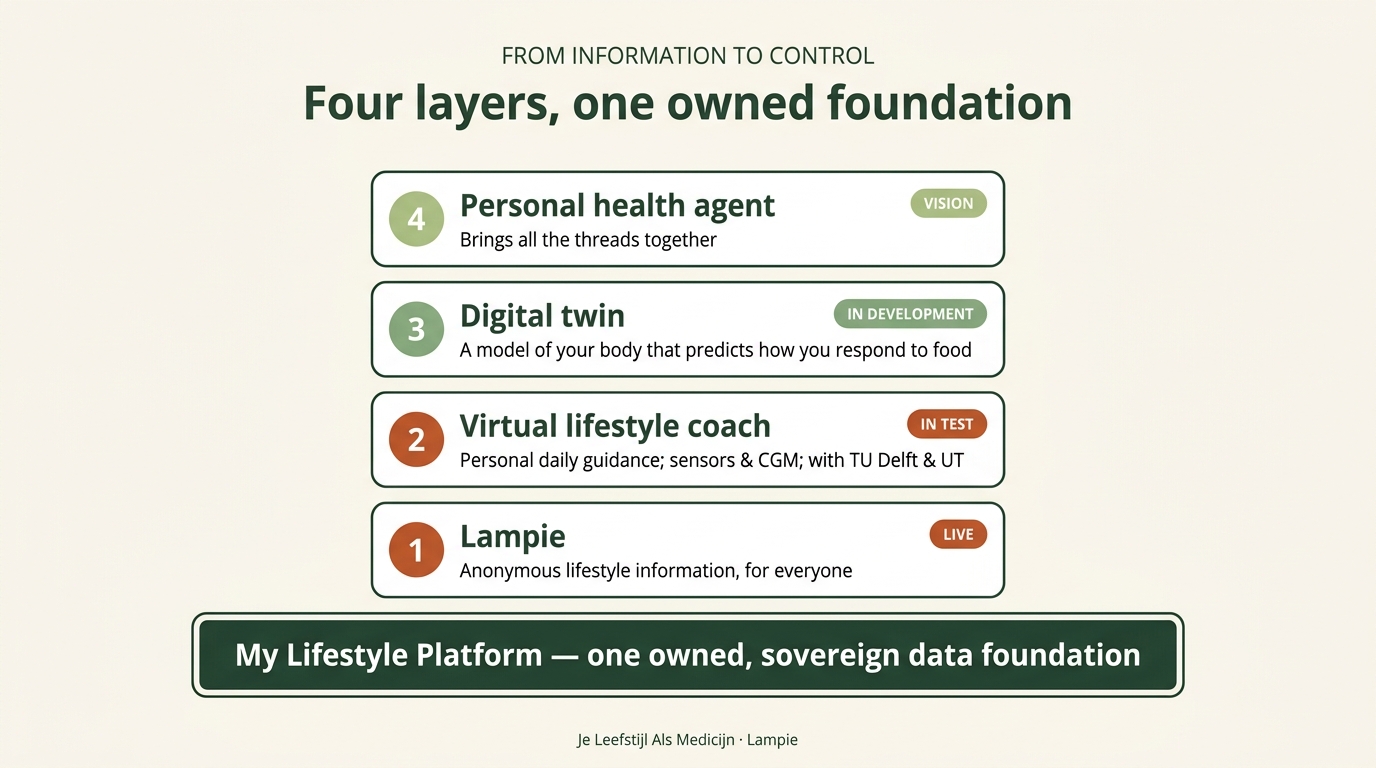
Underneath that whole staircase lies one foundation — and it doesn’t start with technology but with that ZWEM habit: citizens producing their own science. We’re now scaling that measuring culture into one real platform: the My Lifestyle Platform, built by Stef Spooren and Yung Fu, with privacy by design — developed with TU Eindhoven, continued with Radboud University and HU University of Applied Sciences Utrecht.
And notice the circle: for that data foundation exactly the same Golden-Cage logic applies as for the models. An owned, sovereign platform isn’t a detail — it’s the difference between data that belongs to people themselves, and data that ends up in a tech giant’s cage.
9. What’s really happening here
In 2017 TNO researcher Ben van Ommen — the scientist who wrote the blueprint for lifestyle medicine and stood at the cradle of everything described here — called an AI lifestyle coach “the technology that’s almost here”. Almost. Eight years later that coach stands in a hospital waiting room, answers more than 15,000 questions in eleven languages, and its successor is learning to know you personally.
Let me be honest about what Lampie is and isn’t. It cures no one. It replaces no doctor, no dietitian, no walking group. What it does is smaller and at the same time more fundamental: it gives someone at eleven at night a reliable answer and a nudge towards the first step — and connects that person to the knowledge, the people and the places that can walk the rest of the way.
But the architecture underneath carries a bigger conviction. A rented model on someone else’s cloud is comfortable until the moment you realise your healthcare is sitting in someone’s Golden Cage. Our own models, our own data, our own platform — that’s not a technical hobby. It’s the only way “in charge of your own health” also truly means: in charge of your own data.
The future of healthcare isn’t built in hospitals. It’s built by people who take control — supported by science, carried by community, and accelerated by AI we keep in our own hands.
Sources
This piece is built on public sources. I’ve listed them below — grouped, with the people who feature in this story and their roles — so you can read and check everything yourself. Lampie is a product of the Je Leefstijl Als Medicijn foundation, built in partnership with the Dutch AI startup AI voor Impact.
About Lampie — Je Leefstijl Als Medicijn
- Meet Lampie — what Lampie is, where the name comes from and why we built it (in Dutch).
- How Lampie works — the technology under the hood: the knowledge sources, quality assurance and EU AI Act compliance.
- Lampie on your website — the offering for hospitals and care institutions.
Lampie in practice — the hospitals and clinics
- Elkerliek, frontrunner in digital lifestyle support — interview with Elske Berkvens, care-innovation lead at the Elkerliek hospital in Helmond (originally a physiotherapy scientist), on the eleven months to the first hospital go-live.
- Lampie at DC Klinieken — the lifestyle page where Lampie has run in twelve languages since 1 June 2026.
- DC Klinieken on LinkedIn: the announcement by DC Klinieken itself and the post by Lian Tjon Soei Len — medical lead Health & Lifestyle and anaesthesiologist-pain specialist at DC Klinieken.
- The rollout at DC Klinieken is led by Cecile Goldman-Corbeij, director of Innovation & Digitalisation, and Lian Tjon Soei Len.
The next layers
- Virtual lifestyle coach — test programme — the personal coach app now being tested with users.
Model & science
- Deloitte Center for Health Solutions, Smart Health Communities and the Future of Health (2019) — the model that describes the five building blocks.
- Raad et al., BMJ Nutrition, Prevention & Health (2025) — the peer-reviewed study behind the numbers: 232 participants, on average −7.3 kg, without medical supervision.
- Ben van Ommen: the architect of the blueprint — the portrait on this site (in Dutch) of the TNO systems biologist who laid the scientific foundation under lifestyle medicine. He described the AI lifestyle coach back in 2017 and, with his Frontiers review (2018), delivered the blueprint that both JLAM and Lampie build on. Without that blueprint this story wouldn’t exist.
Written by Wim Tilburgs and Claude.